Anxiety and Panic Disorders in Canada: Symptoms, Causes, and Why Rates are Rising
By Rachel Urbas | Certified MHFA Instructor & Psychoeducational Facilitator > Fact-checked & Updated: April 2026

Is anxiety becoming more common in Canada? Recent data suggests a resounding yes. Currently, one in four Canadians will meet the criteria for an anxiety disorder in their lifetime (MHRC, 2020), making them the most prevalent mental illnesses in the country.
Since 2012, cases of Generalized Anxiety Disorder (GAD) have doubled (Statistics Canada, 2022). Understanding the difference between chronic worry and the acute physical intensity of Panic Disorder is essential for those seeking effective treatment as diagnosis rates continue to climb across Canada.
Why is Anxiety Rising in Canada? Understanding the 2024 Statistics
Anxiety disorders are responsible for considerable disability and negatively impact a person’s ability to function in work, school, and social settings.
The rapid increase in diagnoses, particularly since 2012, is a call to action.
The prevalence of Generalized Anxiety Disorder doubled in the last decade.
Generalized Anxiety Disorder (GAD) Doubled: The 12-month prevalence of Generalized Anxiety Disorder (GAD) among Canadians aged 15 and older doubled from 2.6% in 2012 to 5.2% in 2022 (Statistics Canada, 2023).
Anxiety rates for young women (15-24) have tripled since 2012.
The Youth and Gender Crisis: The rise in anxiety is most pronounced among youth and young women. Young women aged 15 to 24 experienced the steepest increase in GAD, with rates nearly tripling (from 3.8% to 11.9%) between 2012 and 2022 (Statistics Canada, 2023).
Women are twice as likely as men to be diagnosed with an anxiety disorder.
Overall, women are consistently about twice as likely as men to be diagnosed with a mood or anxiety disorder in Canada.
25% of the population will meet the clinical criteria for an anxiety disorder at some point in their lifetime.
Specific Prevalence: One in four Canadians (25%) will meet the criteria for an anxiety disorder in their lifetime. Among these various types, Generalized Anxiety Disorder (GAD) is particularly common, with an estimated 13.3% of people experiencing it. Meanwhile, Panic Disorder, characterized by recurrent, unexpected panic attacks, has a lifetime prevalence of around 3.7% (Statistics Canada, 2023).
The Social Media Feedback Loop: Anxiety in Youth

The dramatic rise in anxiety among adolescents and young women is strongly linked to the ubiquity of social media. Research indicates that the time spent on these platforms is a significant predictor of mental distress, especially among girls, whose GAD rates have tripled.
The Mechanisms Driving Distress
While the link between social media and mental health is clear, the distress is driven by a specific set of psychological and biological triggers. These mechanisms create a self-reinforcing loop that keeps the brain in a state of high alert.
Upwards Social Comparison
Platforms like Instagram and TikTok expose users to curated, highly unrealistic versions of their peers' lives, leading to constant and often damaging upward social comparison. This encourages feelings of inadequacy, low self-esteem, and social anxiety.
Fear of Missing Out (FOMO)
The perpetual availability of social interaction creates intense pressure to remain constantly engaged. FOMO drives compulsive checking behaviour, disrupts sleep, and keeps the brain in a perpetual state of hyper-arousal, contributing directly to chronic anxiety.
Cyberbullying and Digital Harassment
Social media is a major vector for harassment. For young people, particularly girls, exposure to cyberbullying significantly increases the risk of developing anxiety and depressive symptoms, often resulting in avoidant behaviours that mirror phobias.
Sleep Deprivation
Using devices late at night inhibits the production of melatonin (the sleep hormone), leading to chronic sleep deprivation. Sleep loss severely impairs the brain's ability to regulate mood and emotion, making the Amygdala (the brain's fear centre) more reactive and making generalized anxiety worse.
Physical Symptoms of a Panic Attack: Why It Feels Like a Medical Emergency
A hallmark of a panic disorder is the sudden, intense panic attack, which involves a terrifying surge of discomfort that peaks within minutes. The experience is often so visceral that it mimics a medical emergency, leading many sufferers to believe they are having a heart attack or stroke.
Physical Symptoms (Fight-or-Flight Response)
The primary symptoms are directly linked to the activation of the sympathetic nervous system (the "fight-or-flight" response) and include:
❤️ Cardiovascular (The Heart): Racing heart, palpitations, or a pounding sensation in the chest. This is the primary reason panic is confused with cardiac distress.
🫁 Respiratory (The Breath): Shortness of breath, "air hunger," or the sensation of smothering and choking.
🌡️ Somatic (The Body): Excessive sweating, trembling, dizziness, and feeling faint or unsteady.
🧠 Psychological: An overwhelming, "doom-like" fear of losing control, "going crazy," or imminent death.
Extreme Neurological and Dissociative Symptoms
The panic response is highly variable and can lead to complex neurological and sensory symptoms that are often missed in mainstream descriptions. These symptoms occur because hyperventilation and extreme adrenaline cause blood vessel constriction (vasoconstriction), reducing blood flow to the extremities and the brain's non-essential areas:
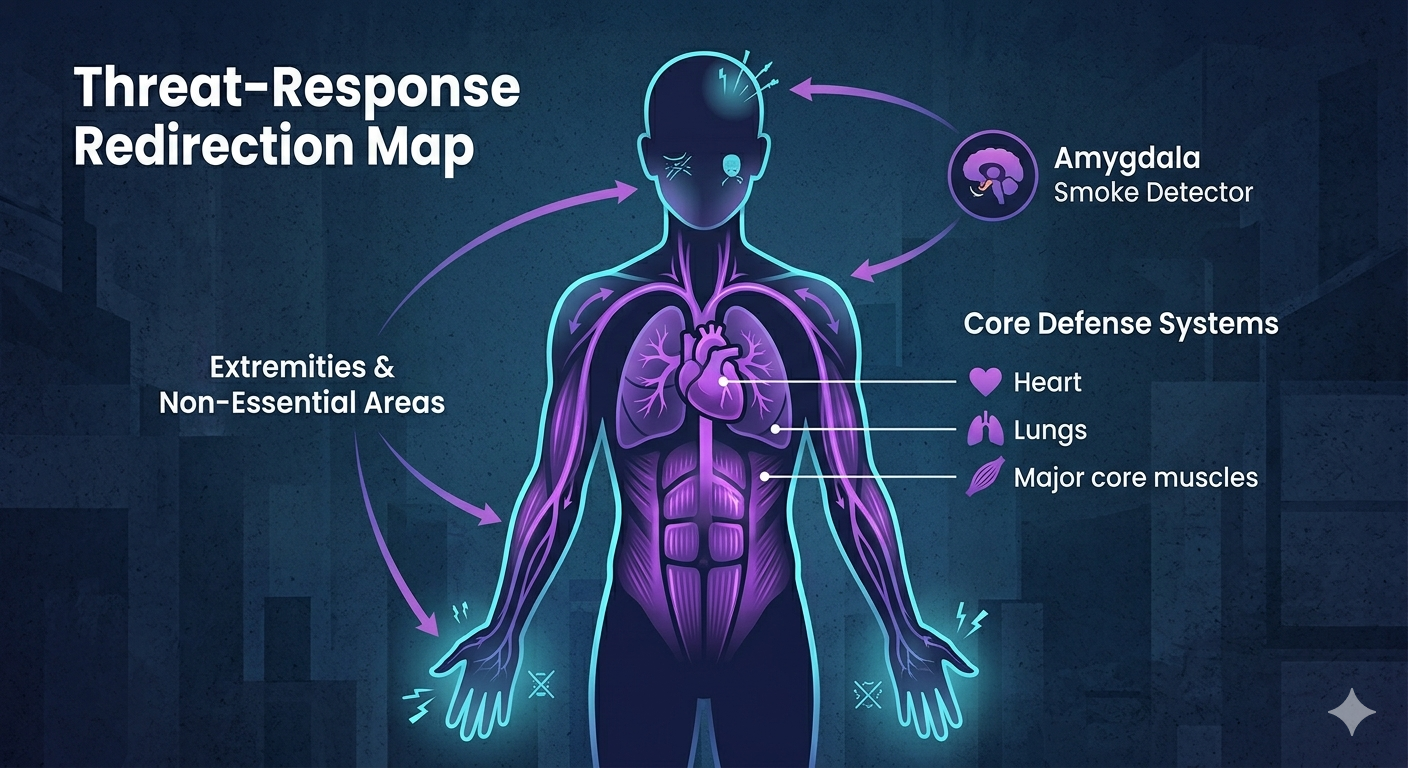
Paresthesia and Numbness: Tingling, prickling, or intense numbness (known as paresthesia) in the hands, feet, face, and head, which can lead to the severe feeling of an oncoming stroke or neurological crisis.
Vision Loss/Disturbances: Temporary changes in vision, such as blurriness, tunnel vision, or momentary vision loss (lasting seconds to a minute). This can be triggered by extreme changes in blood pressure, adrenaline, or anxiety-induced migraine.
Derealization and Depersonalization: A profound, frightening sense of detachment from reality (derealization) or feeling detached from one's own body (depersonalization). These dissociative symptoms are terrifying and contribute to the fear of "losing control".
The Critical Difference: GAD vs. Panic Disorder
While both disorders involve anxiety, they differ fundamentally in focus, intensity, and duration. Misdiagnosis often occurs when the two are conflated.
Generalized Anxiety Disorder (GAD)
Nature of Worry
+Focus of Worry
+Intensity
+Somatic Symptoms
+Onset
+Panic Disorder
Nature of Worry
+Focus of Worry
+Intensity
+Somatic Symptoms
+Onset
+A person with GAD worries constantly about future problems (e.g., losing their job). A person with Panic Disorder is primarily worried about the imminent physical symptoms of having another panic attack.
The Neurobiological Mechanism: Why Panic Feels Like a Physical Threat
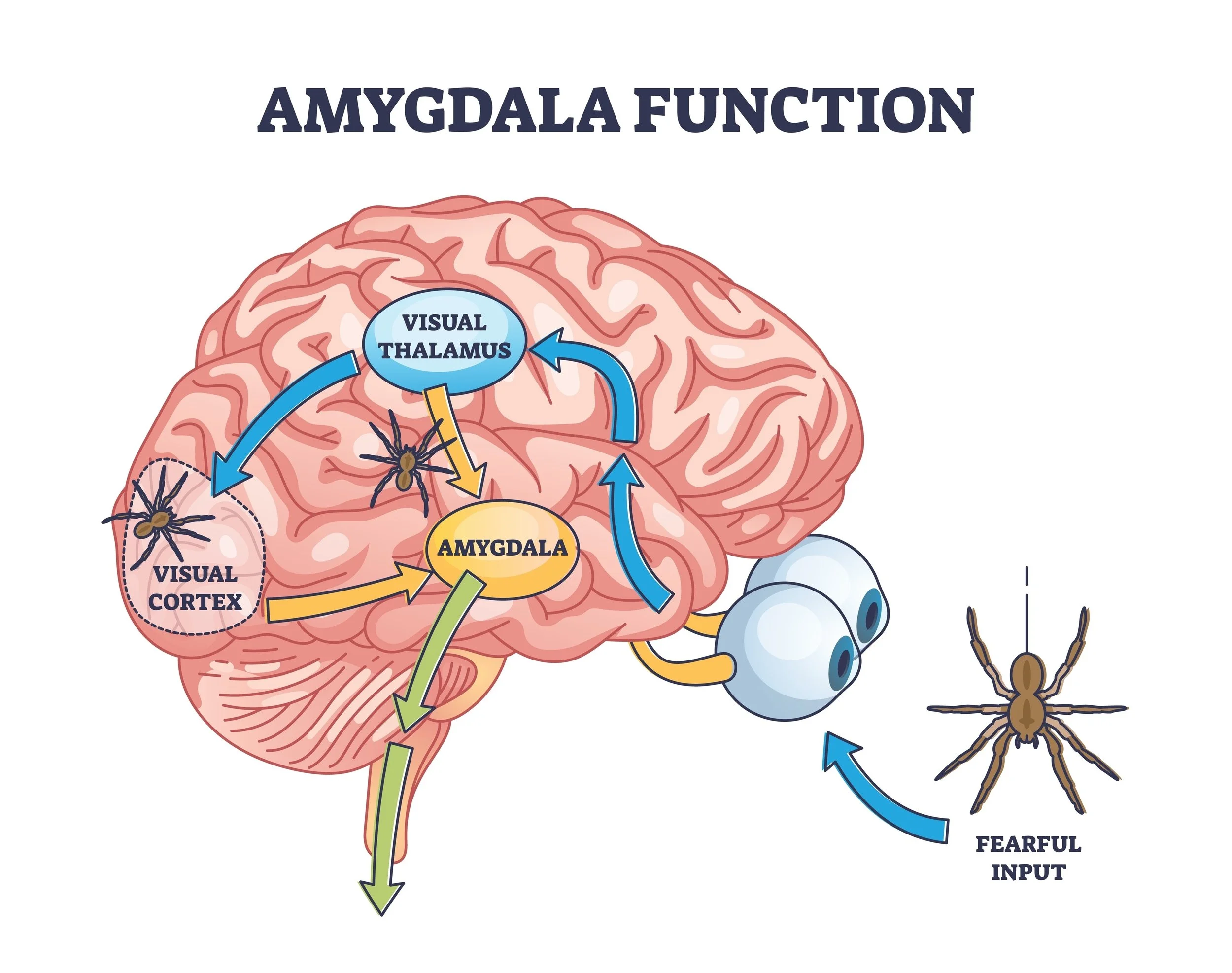
Anxiety disorders, like Substance Use Disorder, are rooted in complex neurobiology. The main biological driver is the Amygdala, the brain's central fear-processing hub.
The Amygdala's Role
The Amygdala acts like a smoke detector. In people with anxiety disorders, this alarm system is often set to an over-sensitive frequency. It can be triggered by real external threats or internal signals, such as a slight increase in heart rate.
Interoception: The Body's Internal Alarm
A key factor that distinguishes panic disorder is a phenomenon known as Interoception: the sense of the internal physiological condition of the body.
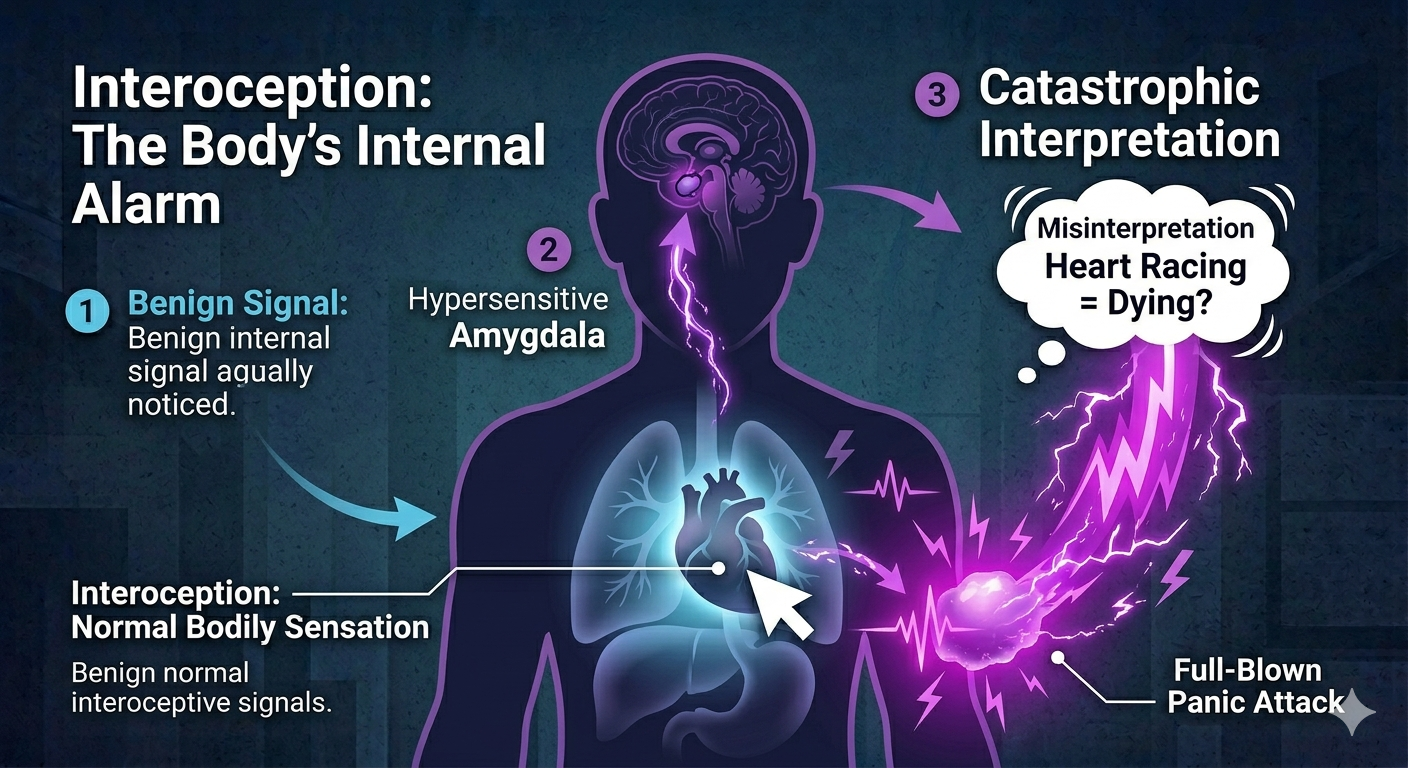
People with panic disorder often display heightened interoceptive attention—they are excessively focused on internal body signals (like heartbeats, breathing rate, or stomach tension).
When a benign sensation occurs (e.g., a natural quickening of the heart from climbing stairs), the hyper-vigilant Amygdala is triggered. The person then catastrophically misinterprets this signal (e.g., "My heart is racing; I must be dying").
This catastrophic belief unleashes the massive, physical panic attack, completing the self-fulfilling cycle where the initial harmless bodily signal (interoceptive cue) creates the full-blown, terrifying physical experience of panic.
The Prefrontal Cortex: The Broken Brakes
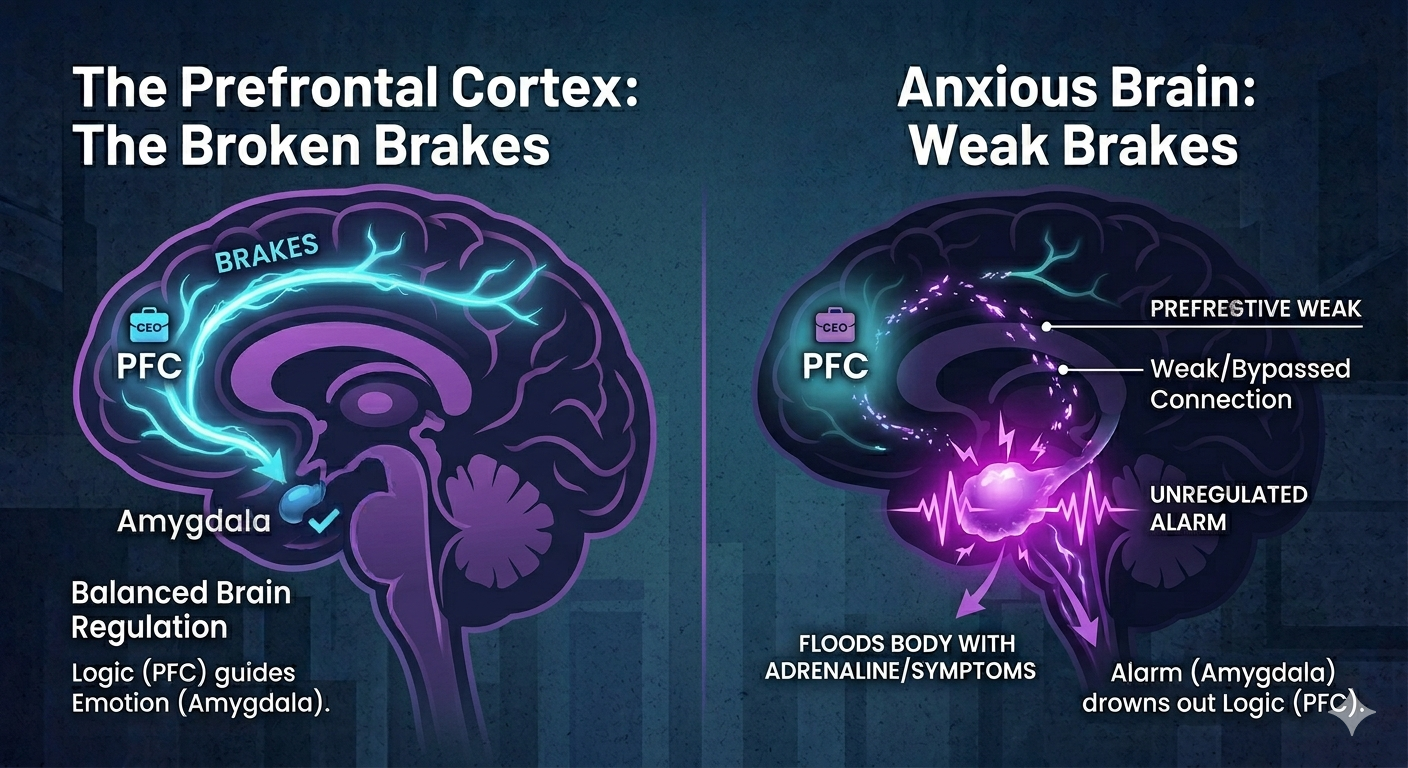
If the Amygdala is the smoke detector, the Prefrontal Cortex (PFC) is the "CEO" of the brain. Located right behind your forehead, this is the part of the brain responsible for logic, reasoning, and calming you down.
In a balanced brain, when the Amygdala screams "DANGER!" because your heart skipped a beat, the PFC looks at the situation and says, "It’s okay, we just drank too much caffeine," and sends a signal to shut the alarm off.
The "Communication Gap"
In anxiety and panic disorders, this "Top-Down" regulation is impaired. The neural pathways (the wiring) between your logical CEO and your emotional Smoke Detector become weak.
The Override: The Amygdala is so loud and fast that it physically "hijacks" the brain before the logical PFC even has a chance to speak.
The Result: You know logically you aren't dying, but you feel like you are because your logical brain has been temporarily unplugged from your physical response system.
Evidence-Based Pharmacotherapy: The Role of SSRIs
While psychotherapy, particularly CBT, is essential, Medication-Assisted Treatment (MAT) is often required to stabilize brain chemistry and provide relief, especially for severe or chronic GAD and Panic Disorder.
Selective Serotonin Reuptake Inhibitors (SSRIs)
SSRIs are the first-line pharmaceutical treatment for most anxiety disorders due to their strong efficacy and safety profile.
Mechanism of Action: SSRIs work by increasing the concentration of the neurotransmitter serotonin in the synaptic gap of the brain. Serotonin is often called the "feel-good" or "modulator" chemical.
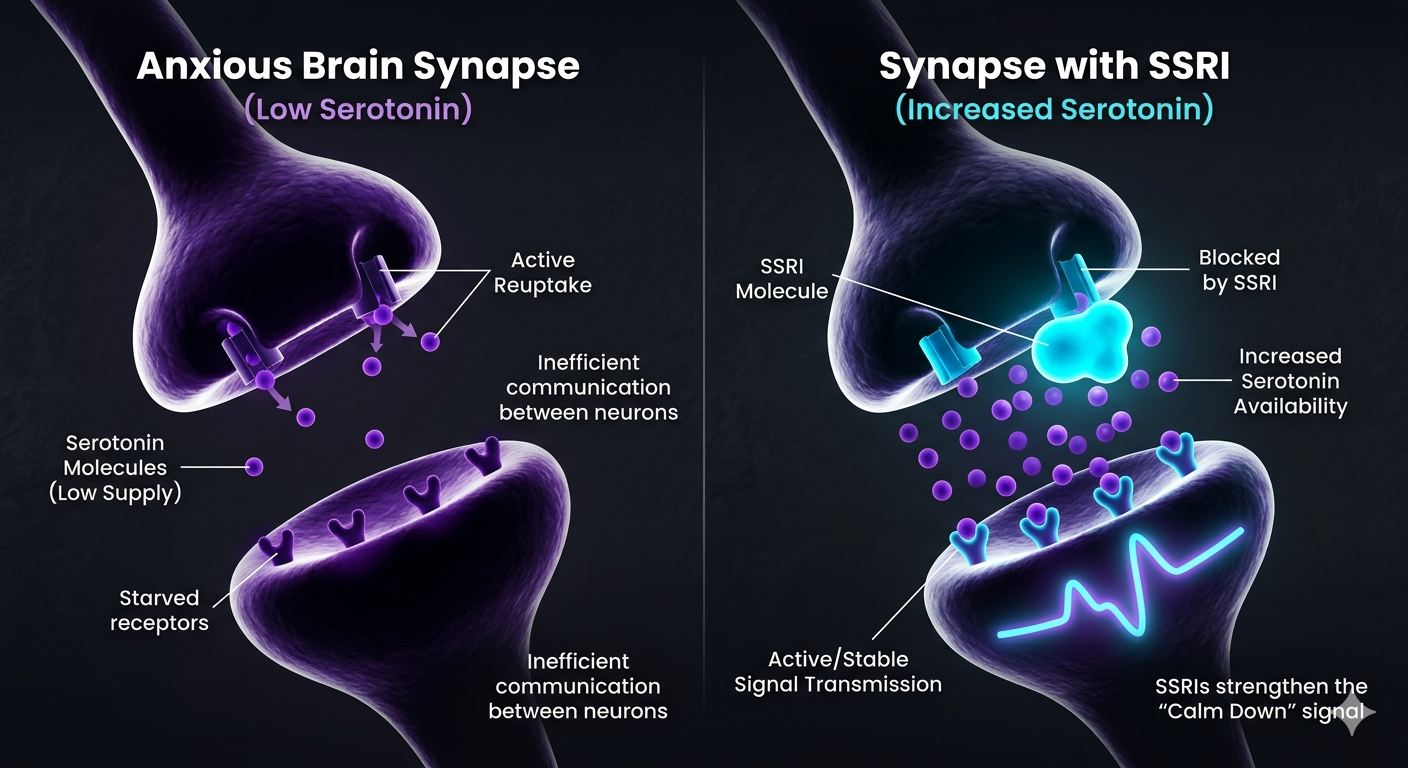
The Desensitization Effect: Through the gentle but persistent increase of serotonin levels, SSRIs help to desensitize the over-reactive Amygdala over several weeks. This dampens the intensity of the "alarm signals," reducing both the chronic, anticipatory worry of GAD and the severity of panic attacks.
Think of medication like brake fluid. If the lines are empty, the signal from the "Logic CEO" (PFC) will never reach the "Alarm" (Amygdala), no matter how hard you press. SSRIs ensure the fluid is there, allowing CBT and therapy to actually work.
Common Examples: Citalopram (Celexa), Sertraline (Zoloft), and Escitalopram (Lexapro). It is crucial for patients to understand that full therapeutic effect may take 4 to 8 weeks, and treatment is a long-term strategy, not a quick fix.
Short-Term Relief: Benzodiazepines
In emergency or severe crisis situations, fast-acting medications like benzodiazepines (e.g., Ativan, Xanax) may be used. However, due to the high risk of dependence and withdrawal severity, these are typically reserved for short-term use during treatment initiation or as a rescue medication for acute panic attacks.
The Systemic Barrier: Cost and The Access Crisis
Despite the severity and widespread nature of these conditions, a major systemic challenge remains the lack of equitable access to care.
Unmet Needs:
Data shows that more than one-third (36.6%) of Canadians who met the criteria for a mood or anxiety disorder reported unmet or partially met health and mental health care needs in 2022 (Statistics Canada, 2023).
The Cost of Effective Treatment:
While Cognitive Behavioural Therapy (CBT) is the gold standard for treatment, publicly funded access remains scarce across Canada. This creates a massive inequity:
The Private Pay Barrier: Canadians are often forced to pay hundreds of dollars per session for private psychotherapy.
The Inequity: High-quality care becomes a luxury, disproportionately impacting low-income and vulnerable populations who cannot afford out-of-pocket costs.
Economic and Social Determinants:
Social determinants of health are not abstract concepts—they are powerful drivers of mental illness. High rates of food and housing insecurity are directly tied to skyrocketing anxiety levels. Currently, 1 in 3 Canadian households (Statistics Canada, 2023) report difficulties meeting basic financial needs, proving that for many, anxiety is a rational response to an unstable economic environment.
Anxiety does not exist in a vacuum. When 1 in 3 households struggle to afford food and housing, mental health is no longer just a neurological issue—it is a social and economic crisis that requires systemic change, not just individual willpower.
Conclusion: The Path to Comprehensive Care
Anxiety and panic disorders in Canada are an escalating crisis rooted in a complex interplay of neurobiological vulnerability, environmental stressors, and a systemic failure to provide accessible, evidence-based care. Addressing this requires a commitment to three specific pillars:
Universal Access
We must move toward establishing publicly funded, easily accessible psychological services—particularly CBT. High-quality mental health treatment should be a right, not a privilege reserved for those who can pay out of pocket.
Integrated Treatment
Recovery is most effective when we combine pharmacotherapy (SSRIs) for biological stabilization with therapeutic intervention (CBT). This dual approach stabilizes the brain's "alarm system" while teaching the prefrontal cortex how to reframe anxious thoughts.
Targeted Support & Digital Wellness
Medical professionals must be better trained to recognize the intense neurological presentation of panic attacks to prevent misdiagnosis. Simultaneously, we must promote digital wellness and sleep hygiene to protect the developing brains of youth from constant environmental overstimulation.
Understanding the Treatment Options
For those seeking relief, understanding which specific evidence-based treatment—such as Cognitive Behavioural Therapy (CBT), Acceptance and Commitment Therapy (ACT), and pharmacotherapy—is the gold standard for managing anxiety and panic disorders is the critical next step.
Anxiety & Panic FAQ
- Statistics Canada (2023). Mental Health and Access to Care Among Canadians, 2022. Findings regarding the 36.6% of Canadians with mood or anxiety disorders reporting unmet or partially met healthcare needs.
- Statistics Canada (2023). Canadian Social Survey: Quality of Life, Cost of Living and Resilience. Data supporting the 1 in 3 Canadian households experiencing difficulty meeting basic financial needs for housing and food.
- Statistics Canada (2020/2022). Trends in Mental Health of Canadian Youth. Documenting the doubling of Generalized Anxiety Disorder (GAD) prevalence among adolescents and young adults over the last decade.
- Mental Health Commission of Canada (2020). Strengthening the Case for Investing in Mental Health Services. Analysis on the clinical and economic efficacy of CBT and the systemic gap in public funding for psychotherapy.
- Harvard Medical School (2023). Understanding the Response to Fear: The Amygdala and the Prefrontal Cortex. Academic overview of the neurobiological mechanics of Panic Disorder and GAD.
Disclaimer: This content is for informational purposes only and does not constitute medical advice, diagnosis, or treatment. Always seek the advice of your physician or other qualified health provider with any questions regarding a medical condition.